lumacaftor
Cystic Fibrosis: Keeping the Momentum Going
Posted on by Dr. Francis Collins
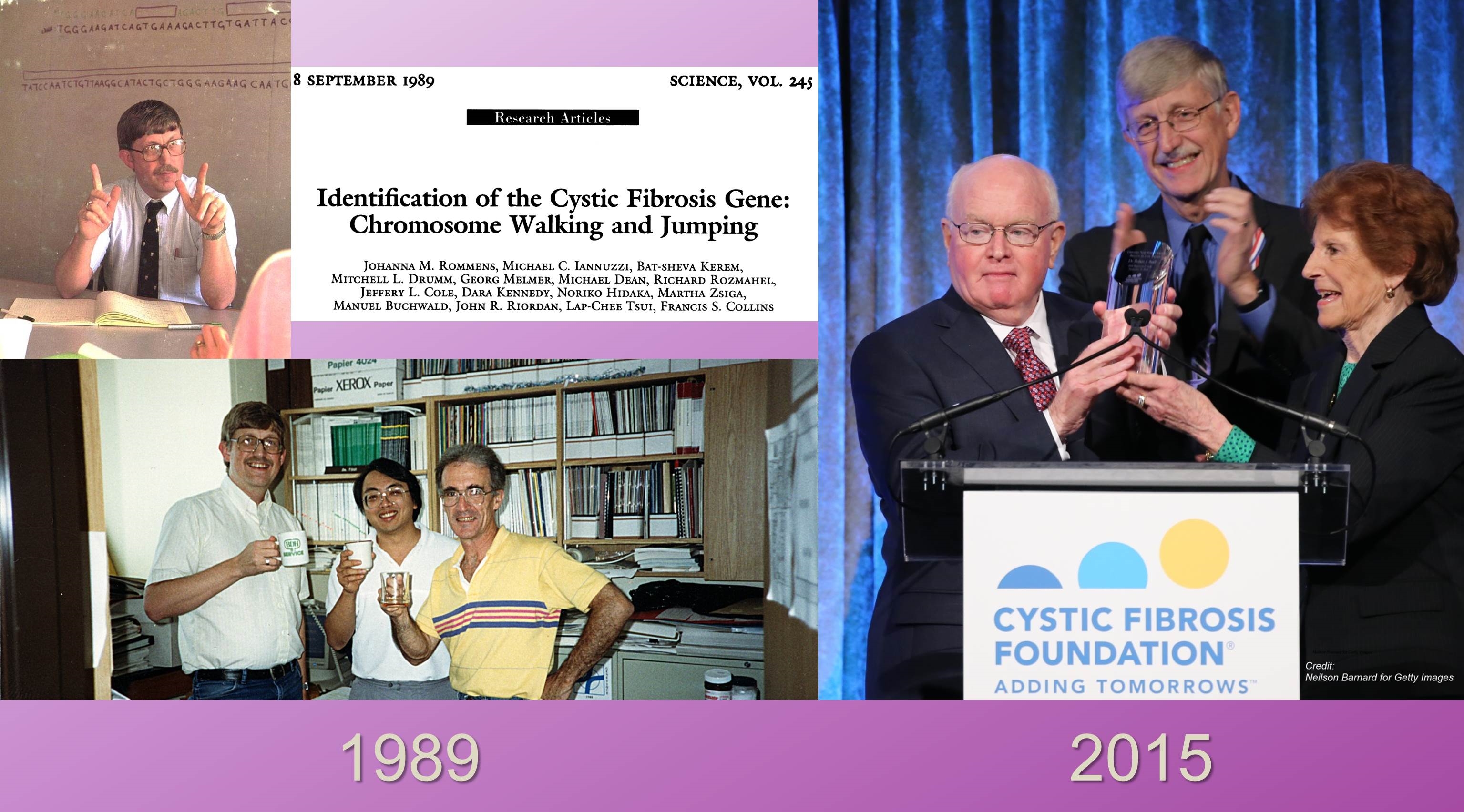
Caption: Lower left, me, Lap-Chee Tsui, and John Riordan celebrating our discovery of the cystic fibrosis gene. Right, Robert J. Beall, me, and Doris Tulcin at a November Cystic Fibrosis Foundation event honoring Dr. Beall.
It’s been more than a quarter-century since my colleagues and I were able to identify the gene responsible for cystic fibrosis (CF), a life-shortening inherited disease that mainly affects the lungs and pancreas [1]. And, at a recent event in New York, I had an opportunity to celebrate how far we’ve come since then in treating CF, as well as to honor a major force behind that progress, Dr. Bob Beall, who has just retired as president and chief executive officer of the Cystic Fibrosis Foundation.
Thanks to the tireless efforts of Bob and many others in the public and private sectors to support basic, translational, and clinical research, we today have two therapies from Vertex Pharmaceuticals that are targeted specifically at CF’s underlying molecular cause: ivacaftor (Kalydeco™), approved by the Food and Drug Administration (FDA) in 2012 for people with an uncommon mutation in the CF gene; and the combination ivacaftor-lumacaftor (Orkambi™), approved by the FDA in July for the roughly 50 percent of CF patients with two copies of the most common mutation. Yet more remains to be done before we can truly declare victory. Not only are new therapies needed for people with other CF mutations, but also for those with the common mutation who don’t respond well to Orkambi™. So, the work needs to go on, and I’m encouraged by new findings that suggest a different strategy for helping folks with the most common CF mutation.
Targeting Cystic Fibrosis: Are Two Drugs Better than One?
Posted on by Dr. Francis Collins

Caption: Doctor with a child with cystic fibrosis who is taking part in clinical research studies. Credit: Colorado Clinical and Translational Sciences Institute
To explain the many challenges involved in turning scientific discoveries into treatments and cures, I often say, “Research is not a 100-yard dash, it’s a marathon.” Perhaps there is no better example of this than cystic fibrosis (CF). Back in 1989, I co-led the team that identified the cystic fibrosis transmembrane conductance regulator (CFTR) gene—the gene responsible for this life-shortening, inherited disease that affects some 70,000 people worldwide [1]. Yet, it has taken more than 25 years of additional basic, translational, and clinical research to reach the point where we are today: seeing the emergence of precise combination drug therapy that may help about half of all people with CF.
CF is a recessive disease—that is, affected individuals have a misspelling of both copies of CFTR, one inherited from each parent; the parents are asymptomatic carriers. The first major advance in designer drug treatment for CF came in 2012, when the Food and Drug Administration (FDA) approved ivacaftor (Kalydeco™), the first drug to target specifically CF’s underlying molecular cause [2]. Exciting news, but the rub was that ivacaftor was expected to help only about 4 percent of CF patients—those who carry a copy of the relatively rare G551D mutation (that means a normal glycine at position 551 in the 1480 amino acid protein has been changed to aspartic acid) in CFTR. What could be done for the roughly 50 percent of CF patients who carry two copies of the far more common F508del mutation (that means a phenylalanine at position 508 is missing)? New findings show one answer may be to team ivacaftor with an experimental drug called lumacaftor.